Balancing Estrogen & Progesterone in Your 30s & 40s

Quick Answer
Hormonal symptoms in women during their 30s and 40s may often be linked to a relative imbalance between estrogen and progesterone rather than excess estrogen alone. Declining progesterone, frequently associated with inconsistent ovulation and hypothalamic-pituitary-adrenal (HPA) axis disruption, can contribute to premenstrual syndrome (PMS), cycle irregularity, and mood changes. Functional hormone testing such as the DUTCH Complete test, combined with targeted nutritional strategies, may help identify and address these shifting hormonal patterns (1–3).
At a Glance
- Progesterone decline from inconsistent ovulation, rather than absolute estrogen excess, may be a primary driver of hormonal symptoms in the late reproductive years (6,7).
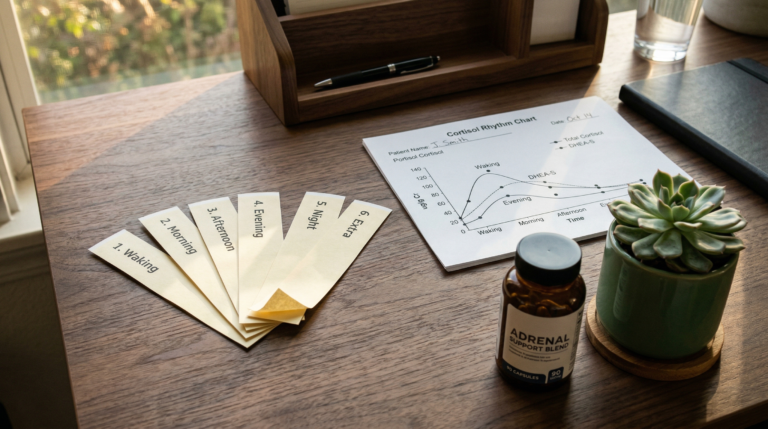
- The DUTCH Complete hormone test measures estrogen metabolites (2-OH-E1, 4-OH-E1, 16-OH-E1), progesterone metabolites, cortisol rhythm, and androgen activity for pattern-based hormonal assessment (9–11).
- Magnesium, vitamin B6, and zinc are cofactors in steroid hormone synthesis and may support progesterone production when adequately supplied (14–16).
- Chronic HPA axis activation can suppress gonadotropin-releasing hormone (GnRH) pulsatility and impair ovulatory function (17,18).
- Soy isoflavones and dietary phytoestrogens may modulate estrogen receptor activity and support hormonal balance during the perimenopausal transition (12).
Estrogen and Progesterone Coordinate Menstrual Cycle Regulation and Systemic Health
Estrogen (primarily estradiol, or E2) and progesterone are steroid hormones produced mainly by the ovaries that work in coordination to regulate the menstrual cycle, mood, metabolism, immune signalling, and reproductive health. According to Reed and Carr (2018), estrogen plays a dominant role during the follicular phase, stimulating proliferation of the uterine endometrium while supporting cognition, tissue repair, and serotonin receptor expression. Brinton (2009) demonstrated that estradiol may also promote synaptic plasticity and neuroprotective pathways in the central nervous system (4,5).
Progesterone, produced by the corpus luteum after ovulation, helps stabilise the secretory endometrium and exerts calming effects on the nervous system via its metabolite allopregnanolone, a positive allosteric modulator of GABA-A receptors. Progesterone also supports immune tolerance and sleep architecture through thermoregulatory effects (4,5).
In an ideal ovulatory cycle, estrogen and progesterone rise and fall in a predictable rhythm across approximately 28 days. However, during the late reproductive years—often beginning in the mid-to-late 30s, as described by the Stages of Reproductive Aging Workshop (STRAW+10) criteria—ovulation may become less consistent. When anovulatory cycles occur, progesterone production declines while estrogen exposure may remain relatively unchanged, creating a relative imbalance (6,7).
This pattern, often described clinically as estrogen dominance, is associated with symptoms including breast tenderness, bloating, fluid retention, menorrhagia, anxiety, irritability, migraines, and sleep disruption. Importantly, Worsley et al. (2021) noted that these symptoms can present even when serum estradiol levels fall within laboratory reference ranges, highlighting the significance of hormone ratios and metabolic clearance rather than isolated values (6–8). These hormonal patterns are commonly explored in functional approaches to mental health and mood regulation.
Functional Hormone Testing May Reveal Patterns That Standard Blood Tests Miss
Conventional serum hormone testing provides a single-point-in-time snapshot and may not capture fluctuations across the menstrual cycle or differences in phase I and phase II estrogen metabolism. For women experiencing cyclical or persistent symptoms, this can lead to results being reported as within reference ranges despite ongoing clinical concerns.
The DUTCH Complete hormone test (Dried Urine Test for Comprehensive Hormones), developed by Precision Analytical, offers a broader view of hormonal patterns. This testing method evaluates multiple analytes across the day and, when appropriate, across the menstrual cycle.
| DUTCH Test Parameter | What It Measures | Clinical Relevance |
|---|---|---|
| Estrogen metabolites (2-OH, 4-OH, 16-OH) | Phase I estrogen detoxification pathway activity | May indicate preferential metabolic routes associated with different symptom profiles |
| Progesterone metabolites (a-pregnanediol, b-pregnanediol) | Luteal phase progesterone output | Can reveal progesterone insufficiency even when serum levels appear normal |
| Cortisol & cortisone rhythm | Diurnal HPA axis activity and cortisol clearance | May identify stress-related disruption of ovulatory function |
| DHEA-S and androgens | Adrenal androgen production | Relevant to polycystic ovary syndrome (PCOS) and adrenal contribution to hormone imbalance |
| Methylation markers (2-MeOE1) | Phase II estrogen methylation via COMT enzyme | May reflect methylation capacity and catechol-O-methyltransferase (COMT) activity |
Rather than focusing on a single hormone value, functional interpretation examines relationships between hormones, their metabolites, and stress physiology. Newman et al. (2019) and O’Donnell et al. (2021) have validated dried urine methodology for steroid metabolite profiling in clinical research settings (9–11).
Targeted Nutritional and Lifestyle Strategies May Support Hormonal Regulation
Once hormonal patterns are identified through functional testing, personalised nutrition and lifestyle strategies may be used to support the systems that regulate hormone production, metabolism, and hepatic clearance. These interventions do not aim to force hormones into balance, but rather to optimise the physiological pathways involved.
| Strategy | Mechanism of Action | Evidence Basis |
|---|---|---|
| Phytoestrogens (flaxseed, soy isoflavones, legumes) | Selective estrogen receptor modulation; may compete with endogenous estradiol at ER-beta receptors | Chen et al. (2015) meta-analysis found soy isoflavones may reduce menopausal symptom severity (12) |
| Seed cycling (flax, pumpkin, sesame, sunflower seeds) | Provides lignans, zinc, selenium, and essential fatty acids across menstrual phases | Limited clinical trial data; may support micronutrient cofactors for steroidogenesis (13) |
| Magnesium supplementation | Cofactor in over 300 enzymatic reactions including steroid hormone synthesis and GABAergic signalling | Nielsen (2010) review linked magnesium deficiency to increased inflammation and hormonal disruption (14) |
| Vitamin B6 (pyridoxal-5-phosphate) | Required for neurotransmitter synthesis (serotonin, dopamine, GABA) and progesterone receptor expression | Dakshinamurti (1993) described B6 roles in neuroendocrine metabolism (15) |
| Zinc | Essential for follicle-stimulating hormone (FSH) and luteinising hormone (LH) signalling, immune modulation | Prasad (2008) demonstrated zinc’s role in immune cell function and endocrine signalling (16) |
Stress Regulation: Chronic activation of the stress response can impair ovulation and reduce progesterone production through effects on the hypothalamic–pituitary–adrenal (HPA) axis. Viau (2002) described functional cross-talk between the HPA and hypothalamic-pituitary-gonadal (HPG) axes, while Berga et al. (1989) demonstrated that psychogenic stress can suppress GnRH pulsatility and induce functional hypothalamic amenorrhoea. Over time, elevated cortisol output may further disrupt estrogen–progesterone balance and worsen symptoms (17,18). This overlap is frequently addressed in functional care for chronic fatigue and low energy.
Moderate Exercise: Regular, moderate physical activity is associated with improved insulin sensitivity, reduced sex hormone-binding globulin (SHBG) variability, and more stable hormonal regulation. De Souza et al. (2010) found that excessive or high-intensity exercise, particularly in the context of low energy availability, may suppress ovulatory function and reduce luteal phase progesterone in some women (19).
All strategies should be individualised and guided by clinical assessment, particularly during periods of hormonal transition.
Signs That May Indicate the Need for Comprehensive Hormonal Assessment
Certain symptom patterns may suggest that a more detailed hormonal evaluation could be beneficial, particularly for women in their 30s and 40s experiencing progressive changes.
| Symptom Pattern | Possible Hormonal Association |
|---|---|
| Increasing PMS severity or new-onset cycle irregularity | Progesterone insufficiency, anovulatory cycles |
| Worsening anxiety, low mood, or reduced stress tolerance | Altered allopregnanolone production, HPA axis dysregulation |
| Sleep disturbance varying across the menstrual cycle | Progesterone-mediated thermoregulatory changes |
| Heavy, painful, or unpredictable periods (menorrhagia, dysmenorrhoea) | Relative estrogen dominance, prostaglandin imbalance |
| Fertility challenges or emerging perimenopausal symptoms | Declining ovarian reserve, follicular phase shortening per STRAW+10 criteria |
Next Steps for Assessing Your Hormonal Patterns
- Track your cycle: Documenting symptoms across your menstrual cycle can reveal hormonal patterns that single-point blood tests may miss.
- Consider functional testing: The DUTCH Complete hormone test evaluates estrogen and progesterone metabolites, cortisol rhythm, and androgen activity for a more complete picture.
- Address stress physiology: Chronic stress is one of the most common disruptors of ovulation and progesterone production—managing it is often a critical first step.
Frequently Asked Questions
Key Insights
- Hormonal symptoms in the 30s and 40s are often driven by relative progesterone decline rather than absolute estrogen excess
- Chronic HPA axis activation and inconsistent ovulation are common contributors to estrogen-progesterone imbalance
- The DUTCH Complete test evaluates estrogen metabolites, progesterone output, cortisol rhythm, and COMT methylation activity
- Magnesium, vitamin B6, and zinc serve as essential cofactors in steroid hormone synthesis and neurotransmitter regulation
- Individualised strategies guided by functional testing are central to safe and effective hormonal support
Citable Takeaways
- Progesterone insufficiency from anovulatory cycles, rather than absolute estrogen excess, may be the primary mechanism behind hormonal symptoms in women aged 30–49, according to Prior (2018) and Fritz & Speroff (2011) (2,6).
- The STRAW+10 staging system (Harlow et al., 2012) established that reproductive ageing and cycle irregularity can begin well before the final menstrual period, with subtle changes often detectable in the late reproductive stage (3).
- Chen et al. (2015) found in a systematic review and meta-analysis that soy isoflavone supplementation may be associated with reduced frequency and severity of menopausal vasomotor symptoms (12).
- Viau (2002) demonstrated functional cross-talk between the HPA and HPG axes, suggesting that chronic cortisol elevation can suppress GnRH pulsatility and reduce downstream progesterone production (17).
- The DUTCH Complete test, validated by Newman et al. (2019), measures estrogen metabolites across three Phase I detoxification pathways (2-OH, 4-OH, 16-OH) and Phase II methylation via COMT, offering a more comprehensive hormonal assessment than single serum values (9).
- De Souza et al. (2010) identified that low energy availability in exercising women may suppress ovulatory function and reduce luteal phase progesterone, contributing to menstrual dysfunction (19).
Move Beyond Isolated Lab Values Toward Pattern-Based Hormonal Insight
A functional medicine approach focuses on identifying hormonal patterns rather than relying on isolated lab values. Comprehensive testing through the DUTCH Complete, combined with targeted nutrition and lifestyle support, may help improve hormonal resilience and symptom management during this transitional life stage. This approach aligns with the broader philosophy of Elemental Health & Nutrition, where patterns are prioritised over single markers.
References
- Santoro N, Randolph JF Jr. Reproductive hormones and the menopause transition. Endocr Rev. 2011 Aug;32(4):513-32. https://doi.org/10.1210/er.2010-0029
- Prior JC. Progesterone for symptomatic perimenopause treatment – progesterone politics, physiology and potential for perimenopause. Climacteric. 2018 Feb;21(1):1-3. https://doi.org/10.1080/13697137.2017.1408784
- Harlow SD et al. Executive summary of the Stages of Reproductive Aging Workshop +10: addressing the unfinished agenda of staging reproductive aging. Menopause. 2012 Apr;19(4):387-95. https://doi.org/10.1097/gme.0b013e318251d8bc
- Reed BG, Carr BR. The normal menstrual cycle and the control of ovulation. In: Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. https://www.ncbi.nlm.nih.gov/books/NBK279054/
- Brinton RD. Estrogen-induced plasticity from cells to circuits: predictions for cognitive function. Trends Endocrinol Metab. 2009 Jun;20(5):212-20. https://doi.org/10.1016/j.tem.2008.12.006
- Fritz MA, Speroff L. Clinical Gynecologic Endocrinology and Infertility. 8th ed. Lippincott Williams & Wilkins; 2011.
- Prior JC. Perimenopause: the complex endocrinology of the menopausal transition. Menopause Int. 2011 Sep;17(3):94-100. https://doi.org/10.1258/mi.2011.011013
- Worsley R et al. Hormones and mental health in women: a review of the evidence. Lancet Diabetes Endocrinol. 2021 Dec;9(12):839-51. https://doi.org/10.1016/S2213-8587(21)00247-3
- Newman MS et al. Dried urine hormone testing methodology: validation and clinical utility. Steroids. 2019 Nov;151:108457. https://doi.org/10.1016/j.steroids.2019.108457
- Reisinger KW et al. Urinary steroid metabolite profiling for diagnosis of disorders of steroidogenesis: development of a novel LC-MS/MS method and clinical utility. Clin Chem. 2020 Jun;66(6):809-18. https://doi.org/10.1093/clinchem/hvaa057
- O’Donnell E et al. Steroid hormone metabolism and urinary analysis: implications for female reproductive health. J Steroid Biochem Mol Biol. 2021 May;209:105848. https://doi.org/10.1016/j.jsbmb.2021.105848
- Chen MN et al. Soy isoflavones and menopausal health: a systematic review and meta-analysis. Climacteric. 2015 Apr;18(2):260-9. https://doi.org/10.3109/13697137.2014.966241
- Cutler WB. Hormonal rhythms and nutritional approaches to the perimenopause. J Womens Health Gend Based Med. 2000 Mar;9(2):119-27. https://doi.org/10.1089/152460900318632
- Nielsen FH. Magnesium deficiency and human health: a review. Magnes Res. 2010 Dec;23(4):S181-90. https://doi.org/10.1684/mrh.2010.0220
- Dakshinamurti K. Vitamin B6 in metabolism and neurobiology. In: Vitamins and Hormones. Vol. 48. Academic Press; 1993:1-45. https://doi.org/10.1016/S0083-6729(08)60500-9
- Prasad AS. Zinc in human health: effect of zinc on immune cells. Mol Med. 2008 May-Jun;14(5-6):353-7. https://doi.org/10.2119/2008-00033.Prasad
- Viau V. Functional cross-talk between the hypothalamic-pituitary-gonadal and -adrenal axes. J Neuroendocrinol. 2002 Jun;14(6):506-13. https://doi.org/10.1046/j.1365-2826.2002.00808.x
- Berga SL et al. Stress-induced reproductive dysfunction: an overview. J Clin Endocrinol Metab. 1989 Nov;69(5):933-8. https://doi.org/10.1210/jcem-69-5-933
- De Souza MJ et al. Energy availability and female athlete triad risk in exercising women: a systematic review. Hum Reprod Update. 2010 May-Jun;16(3):257-74. https://doi.org/10.1093/humupd/dmp050