Optimising Male Health After 40

Quick Answer
After age 40, shifts in testosterone production, cortisol regulation, and metabolic function may contribute to fatigue, weight gain, reduced libido, and diminished stress resilience in men. These changes are not inevitable and are strongly influenced by lifestyle factors including sleep quality, stress exposure, and body composition. Comprehensive hormone and stress physiology assessment, combined with personalised evidence-informed strategies, can help identify contributing factors and guide targeted support.
A structured, functional medicine approach that includes lifestyle foundations and, where appropriate, advanced hormone assessment such as dried urine testing may help clarify the underlying drivers and inform individualised intervention strategies (1-3).
At a Glance
- Testosterone levels may decline by approximately 1-2% per year after age 30, though the rate varies significantly between individuals based on lifestyle and metabolic health (1,2).
- Chronic stress and elevated cortisol can suppress hypothalamic-pituitary-gonadal (HPG) axis signalling, reducing testosterone output (6,7).
- One week of sleep restriction to five hours per night has been associated with a 10-15% reduction in daytime testosterone in young healthy men (16).
- Diurnal cortisol slope flattening is associated with increased cardiometabolic risk and mood disturbance (12).
- Zinc and magnesium are essential cofactors for androgen synthesis and neuromuscular function, and deficiency is common in ageing men (17,18).
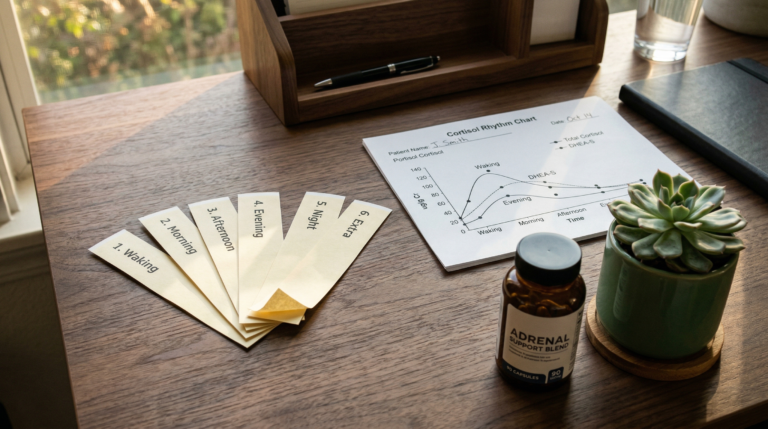
- Comprehensive dried urine hormone testing can assess hormone metabolites and daily cortisol patterns beyond what standard serum testing reveals (13).
Male Ageing, Hormones, and Stress Physiology
Testosterone levels in men decline at an estimated rate of 1-2% per year from approximately age 30 onward, according to longitudinal data from the Baltimore Longitudinal Study of Aging led by S. Mitchell Harman and colleagues (1). From midlife onward, many men experience this gradual decline in circulating testosterone alongside changes in cortisol regulation (4). Testosterone, the primary androgen hormone, is involved in muscle protein synthesis, bone mineral density, mood regulation via serotonin and dopamine pathways, metabolic health, and sexual function (5).
Cortisol, a glucocorticoid produced by the adrenal cortex, plays a central role in the hypothalamic-pituitary-adrenal (HPA) axis stress response and energy regulation. Research by Steven Smith and Wylie Vale at the Salk Institute has established the interconnection between HPA axis activation and reproductive hormone suppression (7).
Chronic psychological or physiological stress can contribute to persistently elevated or dysregulated cortisol output. This pattern has been associated with suppression of hypothalamic-pituitary-gonadal (HPG) axis signalling and reduced testosterone production via gonadotropin-releasing hormone (GnRH) inhibition (6,7). Over time, this cortisol-testosterone interaction may contribute to symptoms frequently reported by men with persistent fatigue and reduced stress resilience, including impaired exercise recovery, mood changes, and increased central adiposity (8).
Importantly, these changes are not uniform. The Massachusetts Male Aging Study, led by Henry Feldman, demonstrated that the degree and pattern of hormonal shift vary widely between individuals, reinforcing the importance of personalised assessment rather than age-based assumptions alone (3).
Common Signs That May Warrant Further Assessment
Multiple overlapping symptoms can indicate age-related hormonal shifts, though each is non-specific and may have alternative explanations. The Endocrine Society clinical practice guideline, authored by Shalender Bhasin and colleagues, recommends comprehensive evaluation rather than symptom-based diagnosis alone (10).
| Symptom | Possible Hormonal Association | Alternative Considerations |
|---|---|---|
| Reduced energy or persistent fatigue | Low testosterone, cortisol dysregulation | Sleep disorders, iron deficiency, thyroid dysfunction |
| Difficulty maintaining lean muscle mass | Declining testosterone, elevated cortisol | Inadequate protein intake, sarcopenia |
| Increased abdominal fat accumulation | Insulin resistance, low testosterone | Metabolic syndrome, dietary factors |
| Reduced libido or sexual changes | Low free testosterone, elevated SHBG | Medication side effects, psychological factors |
| Lower stress tolerance or irritability | HPA axis dysregulation | Anxiety disorders, chronic inflammation |
| Non-restorative or disrupted sleep | Cortisol rhythm disruption | Sleep apnoea, circadian rhythm disorders |
These symptoms may also be associated with sleep disorders, metabolic dysfunction, thyroid dysfunction, or chronic inflammatory states. Hormonal assessment should therefore be considered within a broader clinical context rather than in isolation (9,10).
Hormone and Stress Assessment: Beyond Standard Blood Tests
Standard serum hormone testing measures circulating hormone concentrations at a single time point but may not capture diurnal cortisol rhythm or downstream hormone metabolism through Phase I and Phase II liver pathways (11). William Rosner and colleagues have highlighted the limitations of total testosterone measurement alone, noting that sex hormone-binding globulin (SHBG), albumin-bound testosterone, and free testosterone fractions each provide distinct clinical information (11).
Cortisol secretion follows a circadian pattern regulated by the suprachiasmatic nucleus, typically peaking within 30-45 minutes of waking (the cortisol awakening response) and declining throughout the day. A meta-analysis by Emma Adam and colleagues found that disruption to this diurnal cortisol slope is associated with fatigue, depressive symptoms, and cardiometabolic risk (12).
Comprehensive functional hormone assessments, such as dried urine hormone testing developed by Precision Analytical (the DUTCH test methodology), can provide additional insight into hormone metabolites including 5-alpha and 5-beta reduced androgens, methylation pathways, and daily cortisol patterns. This approach, as described by Shackleton in steroid profiling research, may help clarify how hormones are produced, utilised, and cleared by the body, rather than measuring concentration alone (13). These tests are not diagnostic in isolation and should be interpreted alongside clinical history, symptoms, and conventional pathology results.
When Advanced Hormone Testing May Be Considered
Clinical guidelines from the Endocrine Society and the Australasian Society of Clinical and Experimental Pharmacologists recommend that advanced testing be considered when standard results do not align with clinical presentation (10,14).
| Clinical Scenario | Rationale for Advanced Testing |
|---|---|
| Symptoms persist despite routine blood results within reference ranges | Standard ranges may not reflect individual physiological needs |
| Mismatch between laboratory findings and clinical presentation | Metabolite analysis may reveal downstream processing issues |
| Stress-related symptoms coexist with metabolic or sleep disturbances | Cortisol rhythm mapping can identify HPA axis dysregulation patterns |
| Detailed assessment of androgen metabolism is clinically relevant | 5-alpha reductase activity and aromatase conversion patterns affect symptom presentation |
In some cases, this may include consideration of advanced adrenal and hormone assessments such as the DUTCH Complete hormone test, when clinically appropriate and interpreted by a qualified practitioner (14). David Handelsman of the ANZAC Research Institute has emphasised the importance of contextual interpretation when assessing testosterone levels in clinical practice (14).
Evidence-Informed Strategies to Support Hormonal Health
Research supports a multi-domain approach to maintaining hormonal health in ageing men, with the strongest evidence for interventions targeting stress regulation, sleep, nutrition, exercise, and targeted supplementation.
Stress Regulation
A systematic review and meta-analysis by Michaela Pascoe and colleagues, published in the Journal of Psychiatric Research, found that mindfulness-based practices, diaphragmatic breathing techniques, and deliberate recovery time can measurably influence salivary cortisol levels and perceived stress scores (15). Heart rate variability (HRV) biofeedback may also support parasympathetic nervous system activation and cortisol modulation.
Sleep Optimisation
Rachel Leproult and Eve Van Cauter at the University of Chicago demonstrated in a JAMA study that just one week of sleep restriction to five hours per night was associated with a 10-15% reduction in daytime testosterone levels in otherwise healthy young men (16). Sleep duration, sleep architecture, and circadian rhythm alignment are closely linked to testosterone production, growth hormone secretion, and insulin sensitivity.
Nutrition
Adequate protein intake (approximately 1.2-1.6 g/kg body weight), essential fatty acids including omega-3 polyunsaturated fatty acids, and sufficient micronutrients such as zinc and magnesium support androgen production, neuromuscular function, and metabolic health. Ananda Prasad’s research demonstrated zinc’s role in immune function and testosterone synthesis (17), while Mario Barbagallo and Ligia Dominguez have documented magnesium’s importance in age-related metabolic processes (18). Gut health may also play a role in nutrient absorption and systemic inflammation through the gut-hormone axis, making assessment of the gut microbiome relevant in some individuals.
Exercise Prescription
Resistance training, particularly compound movements performed at moderate-to-high intensity, is associated with favourable acute and chronic effects on testosterone, growth hormone, and insulin-like growth factor 1 (IGF-1). In contrast, Anthony Hackney at the University of North Carolina has documented that excessive endurance training volume without adequate recovery may contribute to exercise-associated hypogonadal conditions in some individuals (19).
Targeted Supplementation
Supplementation should be guided by identified deficiencies or functional needs revealed through comprehensive pathology testing and reviewed regularly to ensure ongoing appropriateness and safety. Sarah Geller and colleagues reviewed the evidence for commonly used dietary supplements in hormone health, noting that efficacy varies considerably by individual context (20).
Move Beyond Guesswork
If you are experiencing persistent fatigue, metabolic changes, or reduced stress resilience and want to understand what is driving your symptoms, a functional medicine assessment can help clarify the picture. At Elemental Health and Nutrition in Adelaide, personalised hormone and stress physiology testing is used to guide targeted, evidence-informed strategies for men over 40.
Men experiencing persistent fatigue, metabolic changes, or reduced stress resilience may benefit from a structured health review that considers hormonal, metabolic, and lifestyle factors together. Individualised assessment allows support strategies to be aligned with physiological needs rather than assumptions based on age alone.
Frequently Asked Questions
Key Insights
- Age-related hormonal change is variable and influenced by lifestyle, stress exposure, and sleep quality
- Chronic stress may contribute to dysregulated cortisol output and reduced testosterone signalling via HPG axis suppression
- Symptoms alone are non-specific and require structured clinical assessment aligned with Endocrine Society guidelines
- Advanced hormone testing such as dried urine profiling can provide additional physiological context but should not replace conventional pathology
- Personalised, evidence-informed strategies targeting sleep, stress, nutrition, and exercise are central to sustainable midlife health
Citable Takeaways
- The Baltimore Longitudinal Study of Aging found that serum testosterone declines progressively with age, though the rate and clinical significance vary substantially between individuals (Harman et al., 2001).
- The Massachusetts Male Aging Study demonstrated population-level testosterone decline is influenced by modifiable factors including body mass index, smoking, and chronic illness, not ageing alone (Feldman et al., 2002).
- One week of sleep restriction to five hours per night was associated with a 10-15% reduction in daytime testosterone in healthy young men, according to a University of Chicago study published in JAMA (Leproult and Van Cauter, 2011).
- A meta-analysis of diurnal cortisol patterns found that flatter cortisol slopes are associated with poorer mental and physical health outcomes, including fatigue and cardiometabolic risk (Adam et al., 2017).
- Mindfulness-based interventions can measurably reduce salivary cortisol and perceived stress levels, according to a systematic review of physiological stress markers (Pascoe et al., 2017).
- Excessive endurance training without adequate recovery may contribute to exercise-associated hypogonadal conditions through suppression of the hypothalamic-pituitary-testicular axis (Hackney, 2001).
References
- Harman SM et al. Longitudinal effects of aging on serum total and free testosterone levels in healthy men. Baltimore Longitudinal Study of Aging. J Clin Endocrinol Metab. 2001 Mar;86(3):724-31. https://doi.org/10.1210/jcem.86.2.7219
- Travison TG et al. A population-level decline in serum testosterone levels in American men. J Clin Endocrinol Metab. 2007 Jan;92(1):196-202. https://doi.org/10.1210/jc.2006-1375
- Feldman HA et al. Age trends in the level of serum testosterone and other hormones in middle-aged men: longitudinal results from the Massachusetts male aging study. J Clin Endocrinol Metab. 2002 Feb;87(2):589-98. https://doi.org/10.1210/jcem.87.2.8201
- Veldhuis JD et al. Endocrine control of body composition in aging. Endocr Rev. 2005 Oct;26(6):795-826. https://doi.org/10.1210/er.2004-0025
- Basaria S. Male hypogonadism. Lancet. 2014 Apr 5;383(9925):1250-63. https://doi.org/10.1016/S0140-6736(13)61126-5
- Cumming DC et al. Cortisol and testosterone interactions. J Clin Endocrinol Metab. 1983 Oct;57(4):671-6. https://doi.org/10.1210/jcem-57-4-671
- Smith SM, Vale WW. The role of the hypothalamic-pituitary-adrenal axis in neuroendocrine responses to stress. Dialogues Clin Neurosci. 2006 Dec;8(4):383-95. https://doi.org/10.31887/DCNS.2006.8.4/ssmith
- Kapoor D et al. Erectile dysfunction and testosterone deficiency in men with diabetes mellitus. Diabetes Care. 2007 Jan;30(1):153-8. https://doi.org/10.2337/dc06-1189
- Mullington JM et al. Sleep loss and fatigue: the role of the stress system. Nat Rev Neurosci. 2009 Jun;10(6):393-402. https://doi.org/10.1038/nrn2649
- Bhasin S et al. Testosterone therapy in men with hypogonadism: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2018 May 1;103(5):1715-1744. https://doi.org/10.1210/jc.2018-00229
- Rosner W et al. Utility of total vs free testosterone: a review. J Clin Endocrinol Metab. 2007 Jan;92(1):1-3. https://doi.org/10.1210/jc.2006-2105
- Adam EK et al. Diurnal cortisol slopes and mental and physical health outcomes: a systematic review and meta-analysis. Psychoneuroendocrinology. 2017 Sep;83:25-41. https://doi.org/10.1016/j.psyneuen.2017.05.018
- Shackleton CHL. Profiling steroid hormones and urinary metabolites. Steroids. 2010 Mar;75(3):169-75. https://doi.org/10.1016/j.steroids.2009.12.003
- Handelsman DJ. Interpretation of testosterone testing. Med J Aust. 2019 Jun;210(11):504-509. https://doi.org/10.5694/mja2.50165
- Pascoe MC et al. Mindfulness mediates the physiological markers of stress: Systematic review and meta-analysis. J Psychiatr Res. 2017 Dec;95:156-178. https://doi.org/10.1016/j.jpsychires.2017.08.004
- Leproult R, Van Cauter E. Effect of 1 week of sleep restriction on testosterone levels in young healthy men. JAMA. 2011 Jun 1;305(21):2173-4. https://doi.org/10.1001/jama.2011.710
- Prasad AS. Zinc in human health: effect of zinc on immune cells. Mol Med. 2008 May-Jun;14(5-6):353-7. https://doi.org/10.2119/2008-00033.Prasad
- Barbagallo M, Dominguez LJ. Magnesium and ageing. Curr Pharm Des. 2010;16(7):832-9. https://doi.org/10.2174/138161210790883679
- Hackney AC. Endurance exercise training and reproductive endocrine dysfunction in men: alterations in the hypothalamic-pituitary-testicular axis. Curr Pharm Des. 2001 Mar;7(3):261-73. https://doi.org/10.2174/1381612013397207
- Geller SE et al. Dietary supplements and hormone health: a review. Am J Med. 2015 Sep;128(9):1024-31. https://doi.org/10.1016/j.amjmed.2015.04.025